In emergencies, every second counts, especially when someone is choking. Fire rescue teams are trained to handle such crises effectively, employing the Heimlich maneuver as a primary technique. This article delves into the importance of understanding how fire rescue personnel respond when faced with choking incidents. The following chapters will cover various aspects, starting with the Heimlich maneuver’s significance, then through emergency protocols, the role of CPR, and the training that prepares personnel for these high-stress situations. Together, these insights will foster awareness and contribute to better preparedness during choking emergencies.
Breath on the Line: How Fire Rescue Teams Use the Heimlich Maneuver to Save Choking Victims Amid the Fire
In the chaos of a burning building, where heat and smoke threaten every breath, a choking incident can add a brutal second front to the emergency. The moment a person struggles to speak, cough, or breathe, the scene shifts from a standard rescue to a race against hypoxia. Fire rescue teams carry this sense of urgency into every incident, because choking is a life-threatening airway obstruction that can deprive a person of oxygen in minutes. The core of the response, in most jurisdictions and in most training regimes, remains the Heimlich maneuver, the abdominal thrusts designed to generate a sudden increase in intra-abdominal pressure to expel the object blocking the airway. This technique is not only a crucial tool in a responder’s chest of skills but also a vivid example of how ground-level first aid and professional fire rescue operations intersect when every second matters. The value of the Heimlich maneuver lies not merely in the action itself but in the speed with which it is applied, the clarity of the sequence, and the confidence it gives to both the victim and the rescuers who stand between danger and relief.
To appreciate how this technique fits into a fire rescue context, it helps to think through the moment when a choking victim is located within or near the line of danger. The first task is assessment: recognizing that the person cannot speak, is unable to cough effectively, or shows signs of airway obstruction. In a smoke-filled room, the signs may progress rapidly, but the principle remains the same: a blocked airway demands immediate action. Firefighters and rescue technicians are trained to act with purpose, not hesitation, because delay increases the risk of a full onset of hypoxia. The assessment is followed by a rapid decision: is it safe to perform the Heimlich maneuver in the current environment? Can the rescuer reach the victim without compromising their own safety or the integrity of the incident scene? These questions, while practical, are essential to the chain of survival that guides every move on the ground. In many standard procedures, when the victim is conscious and the airway obstruction is confirmed, the responder proceeds with abdominal thrusts immediately, performing up to five quick, upward thrusts just above the navel, behind the victim, and with a firm grip. The repetition continues until the object is dislodged or the person loses consciousness. The cadence of those thrusts is not arbitrary; it represents a balance between generating enough internal pressure to overcome the obstruction and avoiding unnecessary injury. This balance is the product of years of training, hours of drills, and the steady hand of a professional who understands the anatomy involved and the risks of a high-stakes rescue in a challenging environment.
The specific circumstances of a fire rescue can complicate the execution of the Heimlich maneuver, but they do not negate its necessity. A standard fire scene is a dynamic stage where heat, smoke, limited visibility, and structural instability all compete for attention. Even so, when a choking person is present and the airway is blocked, responders prioritize a controlled, deliberate approach. The officer at the scene may direct a partner to prepare for immediate action while another team member establishes a safer zone where the victim can receive the maneuver. In many cases, the Heimlich maneuver is employed in the safer corridor or outside the most hazardous area, where responders can maintain the correct body mechanics and obtain the best leverage for effective thrusts. The thrusts themselves are a compact sequence of motion: one hand encircling the forearm or supporting the chest while the other hand applies a quick upward pressure just above the navel. The motion is brief, sharp, and performed in a controlled manner so as to minimize the risk of additional injury while maximizing the chance of expelling the obstructing object.
There are, of course, nuances that shape how the Heimlich maneuver is applied in practice. For one, there are occasions when the abdominal thrusts are not appropriate for everyone. In the case of a pregnant person, a large person, or an individual with certain medical conditions, chest thrusts may replace abdominal thrusts to avoid compromising the fetus or causing undue pressure on the abdomen. Some responders also adapt the technique to accommodate the need for back blows or chest compressions depending on the victim’s status. The overarching principle remains clear: act swiftly, but act with a technique that preserves life and minimizes harm. Fire rescue teams train to recognize these variations so they can adjust their approach without breaking the rhythm of the rescue. The emphasis is not on rigid adherence to a single method but on applying the most effective, evidence-based intervention available in the moment. In this sense, the Heimlich maneuver is not merely a reflexive gesture; it is a structured, teachable response that embodies the core ethos of emergency care: assess, act, reassess, and act again if needed.
A critical facet of this chapter’s focus is the transition when the victim’s airway begins to clear or when the obstruction persists. If the object is expelled, the rescuer immediately checks for breathing and asks the victim to cough, monitoring for a return to normal or near-normal respiration. If the object remains lodged or the person becomes unable to breathe, the responder must shift into other lifesaving steps. In the chain of survival associated with fire rescue, this often means beginning CPR if the person loses consciousness. The CPR sequence—chest compressions paired with rescue breaths—continues according to current guidelines from leading organizations and is an essential backstop when airway control fails. The switch from Heimlich to CPR is not a sign of failure but a necessary escalation when the situation dictates that the airway remains compromised or the person has become unresponsive. The resuscitation sequence can be technically intricate, but its success hinges on the same principles that govern the Heimlich maneuver: rapid recognition, decisive action, careful monitoring, and seamless coordination with the rest of the rescue team.
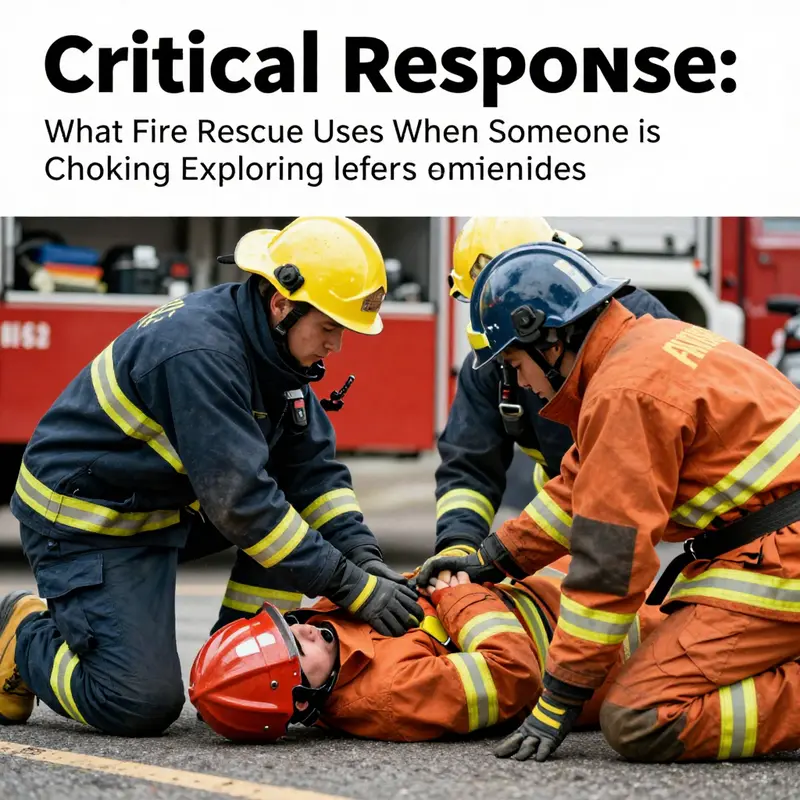
The interplay between choking management and the broader priorities of a fire rescue operation cannot be overstated. Firefighters do not operate in a vacuum; they work within a system of safety protocols designed to protect both life and limb. A choking child or adult in a burning structure, for example, presents a unique challenge: the risk of escalating respiratory distress during removal from the hazard, the potential for dislodging the object while moving through smoke or heat, and the need to ensure that any intervention does not compromise the structural integrity of the environment. In practice, teams may implement additional safety measures, such as stabilizing the patient in a safer area before performing abdominal thrusts, or using a partner to shield the patient from falling debris while the other rescuer applies the maneuver. The procedure thus becomes not just a medical action but a coordinated effort that aligns with overall scene safety, casualty management, and the ongoing demands of the incident command system. This alignment is why the Heimlich maneuver remains a foundational skill in fire rescue training. It represents a clear, decisive tool that can transform a potentially catastrophic moment into a solvable, life-sparing action, even when the clock is ticking and the environment is perilous.
Equally important is the culture and rigor of training that sustains this capability. Fire rescue personnel are trained in basic life support procedures, and choking management is woven into ongoing drills that emphasize accuracy, speed, and situational awareness. The training emphasizes not only the mechanical steps of the procedure but the judgment required to recognize when an intervention is appropriate and when to shift to alternate procedures such as chest compressions or rescue breaths if the victim’s condition deteriorates. In addition to hands-on practice, responders study scenarios that replicate the sensory overwhelm of real incidents: low visibility, loud alarms, the competing demands of equipment handling, and the pressure of maintaining personal safety while delivering life-saving care. The learning approach is holistic, integrating knowledge, psychomotor skills, and the critical thinking that underpins all effective emergency medicine in high-stress environments. This comprehensive preparation helps ensure that when a choking victim is found during a fire rescue, the response is not just technically correct but also timely and harmonized with the broader mission to safeguard life amid danger.
To connect this discussion to practical resources and ongoing learning, many responders look to programs and materials that reinforce the relationship between first aid and the unique challenges of fire rescue work. For readers seeking a more applied understanding of the Heimlich maneuver and its role in immediate airway management, this discussion aligns with practical, experience-based insights from training resources and professional articles. For a deeper dive into the technique and its methodology, a detailed overview is available and can provide a broader scientific context to the procedural steps discussed here. Additionally, those who want to explore related topics in a structured learning path can find related courses and guidance that emphasize safety, preparedness, and the development of a well-rounded emergency response skill set. This chapter’s focus on the Heimlich maneuver and its importance in fire rescue is thus more than a description of a single technique; it is a window into how responders translate foundational first aid into effective action within a complex, high-stakes mission. The capacity to save lives in choking incidents within the fire service is a testament to the power of training, teamwork, and the commitment to protecting every breath that a person has.
For readers who wish to explore additional context about how hands-on techniques are framed within scientific and medical literature, the Heimlich maneuver remains widely discussed as a core intervention for airway obstruction. A recent overview expands on the methodology, its applications, and the conditions under which it remains the preferred initial response. This broader view reinforces the notion that practical rescue work is built on evidence-guided practices that practitioners adapt to field realities. As fire rescue teams continue to refine their approaches, the central takeaway remains consistent: when air is blocked and time is scarce, a trained responder’s confident application of the Heimlich maneuver can change an outcome from tragedy to relief. The human dimension—the calm decision-making under pressure, the trust between team members, and the relief of a recovering airway—remains the heartbeat of every successful intervention in the line of fire.
Internal link to related training resources can enhance a reader’s understanding of how these skills are taught and reinforced in real-world contexts. For a concise look at how safety certification and training practices contribute to preparedness, consider the resource linked here: Fire Safety Essentials Certification Training. This material complements the practical guidance outlined above, offering readers a pathway to deepen their knowledge and contribute to safer outcomes in choking emergencies during fire incidents. By connecting the procedural core of the Heimlich maneuver with the broader framework of professional training, readers gain a holistic view of how modern fire rescue organizations prepare for the unpredictable, always aiming to protect breath and life in the most challenging environments.
External references for further scientific context are available to readers who want to ground these practical discussions in research. For a detailed overview of the Heimlich maneuver and its place in medical literature, see the scientific discussion available at the following resource: Heimlich Maneuver – an overview | ScienceDirect Topics. This external link provides a comprehensive look at the technique, its methodology, and its significance in emergency medical situations that share a common foundation with fire rescue practice.
In sum, the Heimlich maneuver acts as a bridge between urgent airway management and the broader life-saving mission of fire rescue. Its deployment on the fireground—whether in a smoke-filled corridor or a safer assembly area—reflects the discipline, training, and teamwork that define modern rescue work. The technique’s enduring relevance lies in its clarity of purpose, its adaptability to individual circumstances, and its ability to buy precious moments for oxygen delivery. As responders move through the evolving demands of each incident, the priority remains simple and universal: restore breath, secure airway, preserve life, and return to the core work of saving others from the far more visible dangers of fire.
Clearing the Air: How Fire Rescue Teams Manage Choking During an Incident
Rapid assessment and decisive action define how fire rescue teams manage choking during an incident. In a smoky, chaotic scene every second counts. Firefighters arrive trained not only to extinguish flames, but also to preserve life through basic and advanced life support. When a member of the public, a colleague, or an occupant of a structure starts choking, protocols shift immediately to clear the airway. The approach blends simple, proven manual techniques, clear communication, and seamless coordination with emergency medical services.
First, rescuers determine whether the person has a partial or complete airway obstruction. A conscious person who can talk, cough, or breathe is likely experiencing a partial obstruction and may be able to clear the airway on their own. In that case, rescuers monitor and encourage forceful coughing while preparing to intervene. If the person cannot speak, make sound, or is showing signs of severe distress, it is a complete obstruction. Immediate manual intervention follows.
Fire rescue crews are trained to deliver two primary, evidence-based maneuvers to relieve obstruction in conscious victims: back blows and abdominal thrusts. The rescuer positions themselves to maximize effectiveness while ensuring the victim is supported. With back blows, the rescuer stands slightly to the side and behind the person. Using the heel of a firm hand, they deliver up to five sharp blows between the shoulder blades. The intent is to create a sudden change in intrathoracic pressure. That pressure change can dislodge the foreign object.
If back blows do not resolve the obstruction, rescuers move to abdominal thrusts—commonly known as the Heimlich maneuver—for adults and children over one year old. The rescuer stands behind the victim, wraps their arms around the waist, and places a clenched fist just above the navel. The other hand grasps the fist and thrusts inward and upward in quick, forceful motions. Up to five thrusts are given and repeated as necessary. Each thrust aims to raise the diaphragm forcefully, expelling air from the lungs and hopefully dislodging the object.
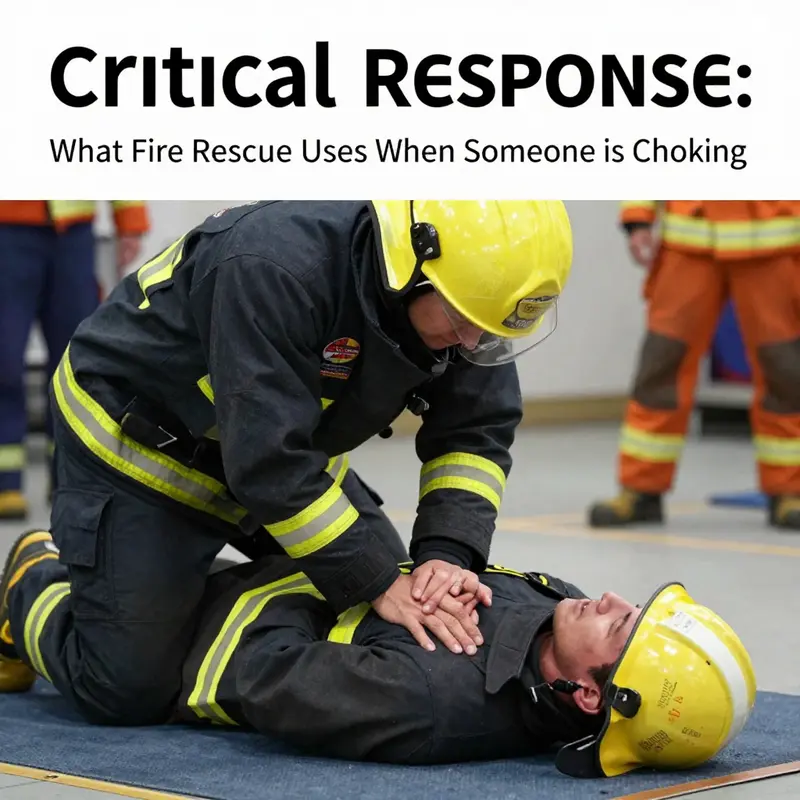
When a choking victim becomes unconscious during a rescue, the protocol shifts to cardiopulmonary resuscitation. Fire rescue personnel begin chest compressions immediately. These compressions are not only intended to maintain circulation, but also can generate enough pressure to expel lodged material. After each set of compressions, rescuers open the victim’s mouth to look for visible obstructions. Any object seen is removed only if it can be easily and safely grasped. Blind sweeps are avoided, as they risk pushing the object deeper.
Fire rescue crews perform cycles of compressions and rescue breaths until advanced care arrives or the person breathes independently. Rescue breaths may be given using pocket masks or bag-valve masks carried on apparatus. These devices protect rescuers from exposure to bodily fluids, a key consideration in the field. Fluid control matters in rescue environments, where smoke, debris, and bodily fluids complicate care.
Managing choking in a fire setting adds layers of complexity. Scene safety is paramount. A rescuer will not expose themselves to untenable hazards like active fire or structural collapse. Yet time-sensitive interventions require balancing safety with the need for rapid airway clearance. Teams often work in pairs: one rescuer secures the scene and maintains safety, while another performs hands-on life-saving maneuvers. This teamwork reduces delays and enhances outcomes.
Special populations require adaptations. For infants under one year old, rescuers use a sequence of five back slaps followed by five chest thrusts with two fingers, instead of abdominal thrusts. For pregnant or obese victims, abdominal thrusts may be ineffective or unsafe; chest thrusts become the alternative. Rescuers position their hands on the center of the chest and deliver rapid thrusts to create sufficient intrathoracic pressure. All procedures follow current best-practice guidelines taught during firefighter medical training.
Equipment carried on fire apparatus supports choking management. Standard medical bags include pocket masks, oropharyngeal airways for unconscious patients, suction devices, and bag-valve masks. When available, advanced airway tools and oxygen can be used by medically qualified personnel. Suctioning can clear fluids or smaller debris obstructing the mouth. Yet, when a foreign body is lodged in the lower airway, manual maneuvers and compressions remain the first-line response.
Documentation and communication are constant components. Crews document the time of intervention, maneuvers used, number of attempts, and victim response. Clear, concise radio reports prepare incoming EMS teams for continuity of care. When handing over the patient, firefighters brief paramedics on whether back blows or abdominal thrusts were performed, if CPR was started, and whether any visible object was removed. That continuity matters for advanced interventions, such as laryngoscopy, intubation, or bronchoscopic removal performed by trained medical personnel.
Legal and ethical considerations are part of training. Fire rescue personnel perform good-faith, standard-of-care procedures when an individual is choking. They operate under protocols and medical oversight. Where available, standing orders and medical director guidance define the scope of practice for various team members. Training emphasizes both the effectiveness of maneuvers and the importance of avoiding harm. Techniques like blind finger sweeps are discouraged because they can worsen obstruction.
Beyond the immediate tactics, fire rescue units emphasize prevention and public education. They teach safe eating practices, supervision of children, and rapid recognition of choking signs. These outreach efforts reduce the incidence of severe airway obstructions and prepare the public to act before trained personnel arrive. For firefighters themselves, regular drills maintain muscle memory for back blows, abdominal thrusts, infant relief sequences, and the transition to CPR if needed.
Response to choking is rarely a solitary act. In a rescue scenario, the chain of survival extends from bystanders to firefighters to paramedics and emergency department teams. Each link strengthens the chances of a positive outcome. Fire rescue teams initiate lifesaving measures quickly. They stabilize the victim. They communicate clearly. They prepare the scene for advanced care.
If you want to learn more about how basic life support skills are taught and certified within the context of fire and rescue work, explore resources on fire safety essentials and certification training. That material explains how these life-saving techniques fit into the broader skill sets firefighters maintain.
For official, in-depth guidance on choking and basic life support, refer to the American Heart Association’s guidelines for Basic Life Support. These guidelines outline the current, evidence-based sequence of actions for choking, CPR, and airway management that fire rescue teams follow in the field: https://www.heart.org/en/residents-and-students/first-aid-and-cpr-guidelines-for-bls
Between Smoke and Breath: How Fire Rescue Teams Tackle Choking with Heimlich, CPR, and Rapid Airway Rescue
In the volatile environment of a fire scene, choking presents a perilous intersection of airway obstruction and hazardous conditions. Fire rescue teams operate under a precise discipline that prioritizes rapid airway relief and, when needed, swift restoration of circulation. The overarching aim is simple in theory but demanding in practice: clear the airway quickly if possible, then sustain oxygen delivery and heart function until skilled medical care can take over. The sequence is built on clear assessment, decisive action, and a readiness to transition seamlessly from one life-saving step to the next as the situation evolves. Firefighters train for the moment when a trapped breath becomes a struggle, and every second matters because the brain’s need for oxygen is unrelenting and unforgiving in smoke-filled environments. The interplay between mechanical techniques, patient monitoring, and the realities of a burning building makes choking management a crucible for skill, teamwork, and calm decision-making under pressure.
For a conscious adult or child who is choking, the primary intervention remains the Heimlich maneuver—abdominal thrusts that generate a sudden increase in intrathoracic pressure to expel the obstructing object. On the fireground, rescuers position themselves behind the person, locate the abdomen just above the navel, and deliver a series of quick, upward thrusts. The goal is not to harm but to create a forceful expulsion that restores airflow while the rescuer maintains contact and communicates with the victim. In many choked scenarios, this rapid sequence is successful in a matter of seconds, allowing breathing to resume and the scene to revert to stabilization rather than prolonged intervention. When the person is an infant, the technique shifts: back slaps and chest thrusts are employed in a careful, staged pattern to protect the infant’s delicate chest and spine while still driving the obstruction outward. The emphasis remains on speed and safety—assessing responsiveness, applying the correct method, and watching for signs that the airway is clearing.
The decision-making process on the fireground hinges on the victim’s responsiveness. If a conscious person can cough forcefully, speak, or breathe with effort, responders monitor closely while continuing to support ventilation and keeping the airway as clear as possible. If coughing wanes or ceases, the rescuer should proceed with the Heimlich sequence, but with an acute awareness that the surrounding conditions—noise, heat, restricted space, and PPE—add layers of complexity. The moment air returns, the airway clears, and the object is dislodged, rescuers transition to a broader assessment. They check for effective ventilation, ensure adequate oxygenation, and prepare for potential secondary injuries that can accompany a stressful event in a hazardous environment. In practice, this means maintaining airway patency, providing supplemental oxygen if available, and remaining ready to escalate to advanced care as needed. In all of this, communications within the team are critical; a coordinated chorus of commands and confirmations keeps everyone synchronized and reduces delays.
When obstruction persists or the victim becomes unconscious, CPR becomes the central lifesaving technique. Fire rescue teams follow the CAB approach—Circulation, Airway, Breathing—because maintaining circulation provides the critical brain and organ perfusion that cannot wait. Chest compressions are initiated immediately, driven by a cadence and depth aligned with current guidelines and adapted to the constraints of PPE and a smoke-filled workspace. After thirty compressions, responders open the airway using the head-tilt/chin-lift maneuver and deliver rescue breaths if trained and equipped to do so, using a barrier device or pocket mask if available. In the field, rescuers also perform a quick check for visible obstruction in the mouth after opening the airway, clearing any object if found before continuing with cycles of compressions and breaths. The aim is to sustain oxygen delivery and circulation long enough to bridge to EMS and hospital care, recognizing that every cycle buys precious time for the brain and vital organs.
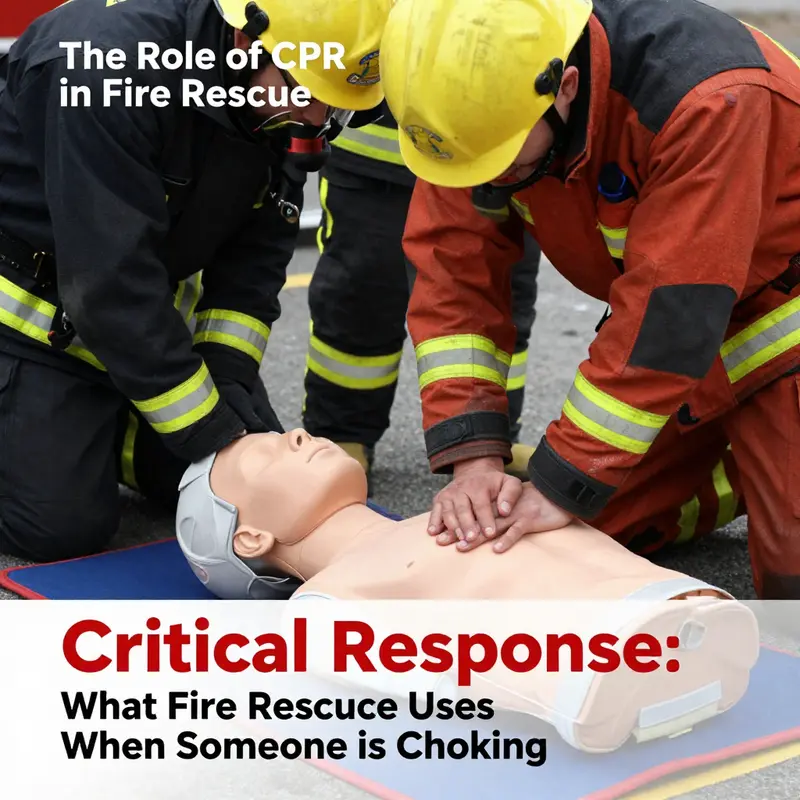
Training provides the backbone for these on-scene actions. Firefighters train with CPR mannequins and high-fidelity simulations that mimic the pressure of a real burning building. Through repeated practice, responders convert knowledge into reflex, enabling rapid, precise maneuvers even while wearing turnout gear, breathing apparatus, and protective equipment. The emphasis on rapid response dovetails with the widely acknowledged “golden four minutes” after cardiac arrest, a benchmark that guides drill design and real-world responses. In practice, this means that rehearsals are engineered to compress typical reaction times, synchronize crew members, and reduce hesitation when airway obstruction or respiratory failure is present. The goal is not simply to memorize steps but to cultivate a shared mental model of how choking can unfold on the fireground, and how to adapt that model to the unpredictable realities of a live incident.
Beyond the mechanics, there is a practical and ethical balance between speed and safety. The rescue environment imposes real risks: smoke irritants, heat, structural instability, and the possibility of additional trauma to the patient. The decision to perform abdominal thrusts, for example, must account for the rescuer’s ability to work safely in PPE and in confined space, the likelihood that the airway is truly obstructed, and whether alternative actions might be more appropriate given the person’s injuries or the building’s conditions. In some cases, responders may adjust their approach to preserve both patient and personnel safety, all while ensuring that the path toward relief of the obstruction remains clear. This thoughtful adaptability—coupled with consistent adherence to established protocols—often determines whether a choking incident ends with recovery or with escalation to more intensive hospital-based care.
The role of airway management extends well beyond mere obstruction removal. Fire rescue units routinely carry devices to support ventilation and oxygen delivery, and they prepare for rapid transition to definitive airway management if necessary. A critical feature of field care is the integration of CPR with airway control, so that once a blockage is cleared, breathing support can continue without interruption. The responders anticipate potential relapse into obstruction and remain ready to employ alternative airway techniques if standard methods prove insufficient. They coordinate with EMS for an orderly handoff, ensuring that patient information, the evolution of the incident, and the synchrony of rescue actions are accurately conveyed to hospital teams. All of this rests on disciplined teamwork, clear lines of authority, and the shared expectation that choking may evolve quickly in the chaos of a fire scene.
The human element of choking response on the fireground deserves attention as well. Each responder brings a matrix of training, muscle memory, and situational judgment to the moment. They must weigh the hazards of smoke inhalation and the potential for trauma against the imperative to restore breathing. The response hinges on a balanced judgment: Was there a true airway blockage? Can Heimlich maneuvers be performed safely given gear and environment? Does forcing airflow risk aggravating an injury, or can safe ventilation be achieved alongside fumigation and heat exposure? Resilience, calm communication, and adherence to protocol turn a high-stress moment into a structured sequence of action. Debriefings, certifications, and ongoing education reinforce this resilience, ensuring that responders keep pace with evolving guidelines and the best available evidence.
For readers seeking a deeper understanding of choking first aid, the Mayo Clinic offers evidence-based guidelines that detail steps for adults and children. While not fire-specific, these principles provide a robust foundation for the logic behind the Heimlich maneuver and the transition to CPR. The documented flow from obstruction relief to resuscitation underscores the universal need to act decisively and systematically when air cannot reach the lungs. Fire rescue training often integrates these general principles with the realities of high-risk environments, ensuring responders can apply them under pressure and within the constraints of their protective gear. For practitioners, these guidelines offer a common frame of reference to coordinate with hospital teams and emergency medical services. External resource: https://www.mayoclinic.org/first-aid/first-aid-choking/basics/art-20056647.
A note on accountability and continuous improvement closes this reflection. Each choking incident on the fireground becomes a learning event: responders review what occurred, what worked, and what did not. They discuss the timing of Heimlich maneuvers, the decision points when to switch to CPR, and the effectiveness of airway management in a smoke-filled space. The goal is not to dramatize the crisis but to distill practical wisdom that strengthens readiness for the next call. Combined with regular drills, debriefings, and certifications, this reflective practice ensures that every firefighter remains prepared for the odds they will face. The chain of survival in choking is a loop that feeds back into training, policy updates, and community education, reinforcing a culture of continuous improvement that serves both responders and those they rescue.
Finally, choking response is inseparable from the broader mission of fire rescue. The techniques and decisions described here illuminate how life-saving skills move from the controlled setting of a classroom into the chaos of real emergencies. The same fundamentals—rapid assessment, clear communication, methodical action, and coordinated teamwork—apply when saving a victim from smoke inhalation or when managing a patient with other injuries. In this sense, the work of fire rescue extends beyond extinguishing flames; it is about preserving breath, protecting the brain, and minimizing time lost when airway—and thus life—hangs in the balance. The integration of discipline, physical readiness, and medical knowledge forms the backbone of a rescue system that can adapt to the most challenging scenarios. For professionals in the field, this continuity between training, on-scene practice, and clinical care is what makes choking management a defining measure of readiness, resilience, and responsibility.
To reinforce the practical tie between training and real-world choking responses, consider that professional development resources emphasize the same core competencies highlighted in this chapter. For example, accessible training modules and certifications cover airway management, CPR, and the critical decision points that determine whether to attempt abdominal thrusts or pivot to chest compressions. This alignment ensures that every responder who trains today will be better prepared to protect a life tomorrow. And as communities grow more aware of fire safety and emergency response, the integration of these skills into public education keeps the chain of survival strong—from the fire station to the street, to the hospital, and back into the community where prevention begins.
null
null
Final thoughts
Fire rescue personnel play a vital role in responding to choking emergencies. Understanding their techniques, particularly the Heimlich maneuver and CPR, can make a significant difference in life-and-death situations. Well-trained personnel equipped with emergency protocols ensure that victims receive timely assistance, demonstrating the importance of regular training and awareness in the community. Preparedness is key, and knowing what to expect from fire rescue can empower individuals and enhance public safety.

